If you’ve ever watched a loved one stumble through another night of missed appointments, empty promises, and whispered apologies, you know the gut‑wrenching feeling of helplessness that comes with addiction. Does it seem like every conversation ends in denial, and the hope you cling to keeps slipping away? In this guide we’ll unpack what a drug intervention really looks like, why it matters, and how you can start moving toward a safer, healthier future for your family.
First, understand that an intervention isn’t a dramatic showdown—it’s a carefully planned, compassionate conversation that brings together people who truly care. Think about the last time you gathered friends for a birthday surprise; you had a plan, you rehearsed what to say, and you made sure the setting felt safe. A drug intervention follows the same script, only the goal is to gently guide the person toward treatment instead of a party.
What we’ve seen work best is a three‑step framework: (1) Assemble a trusted circle, (2) Choose a neutral, private space, and (3) Present clear, non‑judgmental facts paired with treatment options. For example, a mother in Anaheim brought together her brother, a close friend, and a counselor, met at a quiet park pavilion, and calmly shared the impact of her son’s opioid use, offering immediate referrals. That structure gave the conversation focus and prevented the discussion from spiraling into blame.
When you’re ready to take the first step, start by writing down concrete observations—missed work days, mood swings, financial red flags. Next, reach out to a professional who can coach the family through the process; they’ll help you rehearse what to say and handle any emotional blow‑backs. Our own team at Next Step Intervention has guided dozens of families through this exact roadmap, and we can provide a template that outlines talking points and timelines. Drug Intervention services are designed to take the guesswork out of that nervous first meeting.
Remember, recovery doesn’t happen in isolation. Research shows that people who receive timely intervention are 30 % more likely to enter treatment within the first month. Pairing the intervention with supportive lifestyle changes—like improving sleep hygiene—can boost those odds even further. A good night’s rest reduces stress hormones that often trigger cravings, so consider simple upgrades such as breathable bedding. If you’re curious about how a better mattress can make a difference, check out this guide on choosing the coolest bed for better sleep.
So, what’s your next move? Grab a notebook, list the people you trust, and schedule a brief call with an interventionist today. The sooner you act, the sooner your loved one can step onto a path of lasting recovery.
TL;DR
A drug intervention, when planned with a trusted circle and a professional guide, turns chaotic denial into a clear, compassionate path toward treatment and lasting recovery.
Start by noting concrete signs, reach out to an interventionist today, and you’ll give your loved one the support they need to break the cycle and reclaim hope.
Step 1: Assess the Need for a Drug Intervention
So you’ve started to notice the red flags – missed appointments, mood swings, that sudden cash crunch. It feels like you’re watching a loved one drift further away, and you’re left wondering, “Is this the moment to step in, or am I just going to make things worse?” That uneasy feeling is exactly why we begin with a clear assessment. It’s not about labeling; it’s about grounding the conversation in facts you can both see.
First, grab a notebook or a notes app and write down concrete observations. Think of it like a log you’d keep for a car’s maintenance: oil changes, strange noises, warning lights. In the addiction world, your “warning lights” might be a pattern of skipped workdays, secretive phone calls, or unexplained injuries. The more specific you are, the harder it is for denial to hide behind vague feelings.
Next, ask yourself three quick questions:
- What behaviors have changed in the last 30 days?
- How has this affected the family’s daily routine or finances?
- What have I tried already, and what was the result?
Jotting down answers creates a reality check you can refer back to when emotions run high. It also gives you a solid foundation for the next step – bringing in a professional.
And here’s a gentle nudge: don’t try to diagnose yourself. If the pattern feels overwhelming, reach out to an interventionist. In our experience, families who involve a certified professional early on feel more confident and less isolated. A quick call can help you shape the facts into a compassionate script.
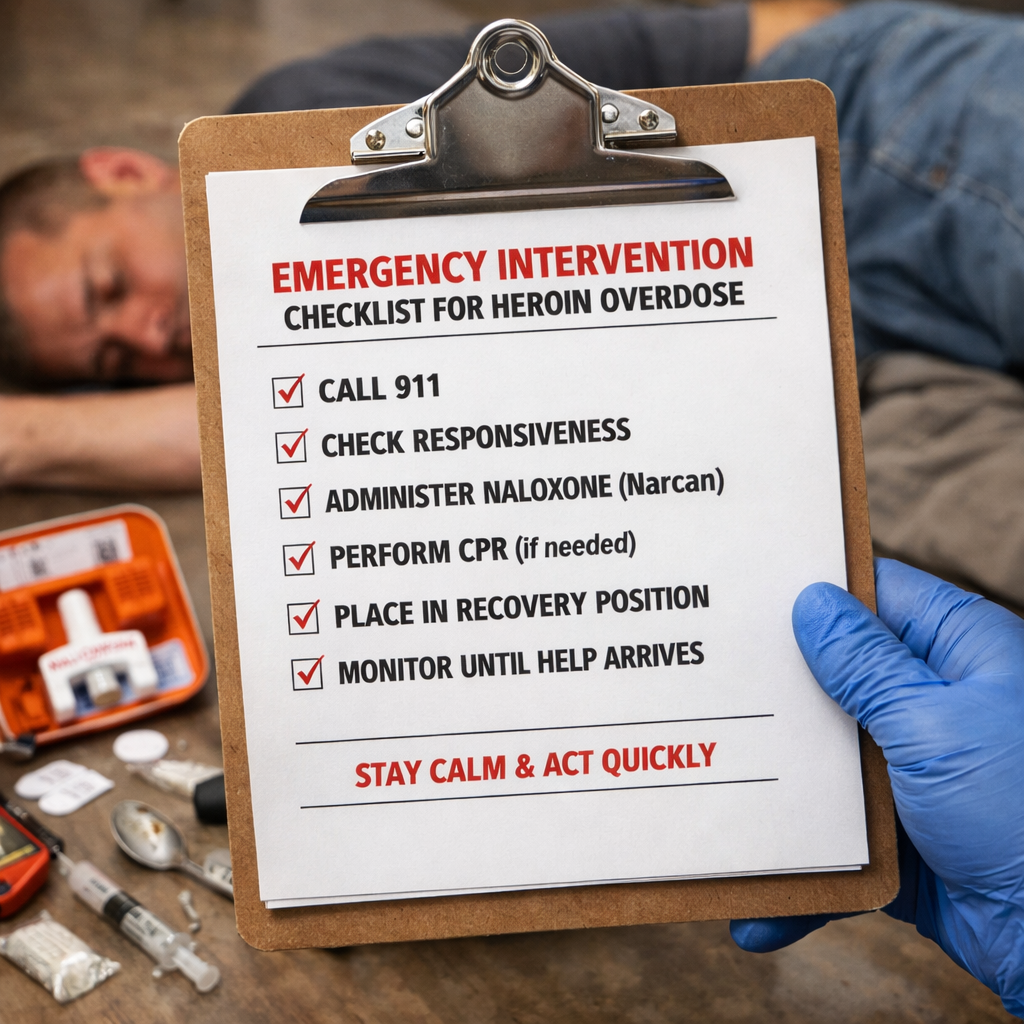
Once you have the list, rank each item by impact – from “minor annoyance” to “potential safety risk.” This ranking helps you decide whether the situation calls for an urgent intervention or a more measured conversation. If you notice any sign of self‑harm, overdose risk, or severe withdrawal, treat it as an emergency and call a medical professional immediately.
Now, let’s talk about the environment. A neutral, private space is key – think of a calm living room or a quiet park pavilion, not the kitchen table where arguments usually happen. The setting should feel safe enough for everyone to speak honestly without feeling judged.
When you’re ready to bring in an expert, you might wonder where to start. Drug Intervention | Intervention Services in California & the … walks you through the process of finding a certified interventionist who can coach you through the conversation, rehearse talking points, and keep the meeting on track.
But a drug intervention isn’t just about the moment you sit down together; it’s part of a larger recovery ecosystem. Good sleep, proper nutrition, and regular wellness check‑ins can dramatically boost the chances of lasting change. That’s why we recommend pairing the intervention with holistic health resources. For example, a comfortable mattress can lower stress hormones that often trigger cravings. If you’re curious about how a cooler bed can help, check out this guide from SleepSophie: Mattress for Hot Sleepers: How to Choose the Coolest Bed for Comfortable Nights.
Another piece of the puzzle is proactive health monitoring. Programs that offer regular wellness assessments can spot early signs of relapse and keep the recovery momentum going. XLR8well provides exactly that kind of ongoing health partnership: XLR8well.
Below is a quick checklist you can print out and fill in as you gather information:
- Date and time of each concerning incident
- Specific behavior observed (e.g., missed work, secretive phone calls)
- Impact on family finances, relationships, or safety
- Any attempts at intervention and outcomes
- Urgency rating (low, medium, high)
Having this checklist handy will make the next conversation feel less like a guessing game and more like a shared problem‑solving session.
Here’s a short video that walks through how to organize your observations and what to look for before you call an interventionist.
Take a moment after watching to add any new insights to your notebook. The act of writing solidifies your observations and makes the next step feel more concrete.

When you’ve completed the assessment, you’ll have a clear picture of why a drug intervention is needed and how urgent it is. The next step will be assembling your trusted circle and planning the conversation, but that’s a story for the next section. For now, trust that this assessment phase is the foundation that turns worry into actionable hope.
Step 2: Choose the Appropriate Intervention Method
Now that you’ve gathered the facts, the next puzzle piece is deciding *how* you’ll present them. The method you pick shapes the tone, the level of confrontation, and ultimately how likely your loved one is to stay engaged long enough to accept help.
There are three main families of drug intervention approaches that families keep talking about: the classic Johnson Model, the CRAFT (Community Reinforcement and Family Training) method, and a hybrid “conversation‑first” style that blends elements of both. Each one has its own sweet spot, and the best choice depends on the person’s age, the severity of use, and how much resistance you anticipate.
Johnson Model – the “direct‑to‑the‑point” plan
Think of this as the “talk‑hard‑but‑loving‑ly” route. You gather a small circle, present the screening scores, and lay out a non‑negotiable treatment offer. The goal is to create a moment of reality shock that cuts through denial.
Real‑world example: Maria’s 45‑year‑old brother was slipping deeper into opioid use after a workplace injury. She and two close friends sat him down in a quiet living room, read his high DAST‑10 score aloud, and handed him a signed intake form for a nearby rehab. Within 48 hours he checked in, saying the “hard line” felt like a lifeline he couldn’t ignore.
CRAFT – the “coach‑and‑reward” approach
CRAFT flips the script. Instead of confronting the user directly, the family learns reinforcement techniques: praising sober behavior, setting clear boundaries, and gradually introducing professional help. It works especially well when the person is highly resistant or when children are in the mix.
Consider James, a single dad whose teenage son was caught with meth at school. James enrolled in a CRAFT training program, learned to replace “you’re always messing up” with “I noticed you finished your homework without any trouble today – that’s awesome.” Over three months the teen’s use dropped enough for a therapist to step in without a dramatic showdown.
Hybrid / Conversation‑First style
Some families find a middle ground useful: they start with a gentle, fact‑based conversation, gauge the reaction, and then pivot to a firmer stance if the person pushes back. This flexibility is handy when you’re not sure how much denial you’ll face.
For example, Lisa’s adult daughter was drinking heavily but still employed. Lisa opened with a calm review of her recent missed work days and the AUDIT‑C score, then asked, “What do you think would help you get back on track?” When the daughter brushed it off, Lisa calmly shifted to the firm offer of an inpatient program she’d already booked.
How to pick the right method for your family
- Age group – Younger adults and teens often respond better to CRAFT’s positive reinforcement; older adults may need the decisive push of the Johnson Model.
- Severity – High‑risk scores (e.g., DAST‑10 ≥ 8) usually merit a more structured, non‑negotiable approach.
- Support network – If you have a strong circle of trusted friends, the Johnson Model’s group pressure can be powerful. If you’re a solo caregiver, CRAFT’s one‑on‑one coaching may be more realistic.
- Legal or employment stakes – When jobs or court dates are on the line, a firm “we have a treatment plan ready tomorrow” tone often wins.
Actionable checklist for choosing your method
- Review the screening score you recorded in Step 1.
- Ask yourself: Is the person likely to accept a gentle nudge or does denial feel entrenched?
- Match the scenario to a model:
- High denial + high risk → Johnson Model.
- Low‑to‑moderate risk + strong family involvement → CRAFT.
- Uncertain reaction → Hybrid conversation‑first.
- Write a one‑page script that includes:
- Key facts (screening score, observed behaviors).
- Your chosen approach (e.g., “We’re here to support you, and we’ve arranged a treatment slot.”)
- Concrete next steps (appointment date, transportation plan).
- Run the script by a certified interventionist. In our experience, a quick review can spot tone issues before the big day.
- Schedule the meeting in a neutral, private space – a living room, a park pavilion, or even a quiet coffee shop if the setting feels safer.
If you’re still unsure which path fits best, our Adult Interventions service walks you through a personalized assessment and recommends the most effective method for your situation.
Take a moment now: grab that notebook, tick off the checklist above, and commit to a method by tomorrow. The sooner you lock in a plan, the less room denial has to grow, and the more momentum you’ll have when the day arrives.
Step 3: Implement the Intervention Safely
Alright, you’ve picked a method and gathered your circle. Now the real test begins: turning that plan into a safe, compassionate moment that actually moves the person toward treatment.
First things first – location matters. You want a neutral, private space where everyone feels heard but no one feels trapped. Think a quiet coffee shop back room, a community center meeting room, or even a living‑room with the TV turned off.
So, how do you make sure the setting stays calm? Here’s a quick checklist:
- Choose a place with easy exits for everyone.
- Make sure the room is well‑lit but not harsh.
- Arrange seating in a circle – no “head of the table” hierarchy.
- Have water and a neutral snack on hand; it reduces tension.
Does any of that sound familiar? It’s the same logic behind the drug market intervention guide that helps law‑enforcement and community partners keep interventions low‑key and high‑impact.
Next, rehearse your script. You’ve already written it in Step 2 – now read it aloud with a friend who isn’t in the intervention. Notice any phrasing that feels accusatory. Swap “You always…” for “We’ve noticed…”. The goal is to keep the tone factual, not judgmental.
Ever wondered why tone is such a big deal? Because the brain reacts to perceived threat faster than to logic. A calm voice can keep the fight‑or‑flight response at bay, letting the person actually hear the facts.
When the day arrives, stick to a simple timeline:
- Arrival: Greet everyone, offer water, and let the person settle for a minute.
- Opening: Share the agreed‑upon facts (screening score, observed behaviors) in a matter‑of‑seconds statement.
- Offer: Present the concrete next steps – a treatment slot, transportation plan, or a follow‑up call.
- Close: Summarize the agreement, hand out a one‑page recap, and set a clear date for the next contact.
Keep each segment under two minutes. If emotions flare, pause, breathe, and gently redirect back to the script.
Safety tip: Assign one person as the “time‑keeper” and another as the “de‑escalation lead.” The time‑keeper watches the clock; the de‑escalation lead watches body language and steps in if voices rise.
Here’s a handy comparison table that captures the core safety elements you’ll juggle during the meeting:
| Safety Element | Action Step | Why It Matters |
|---|---|---|
| Location | Choose a neutral, private room with easy exits. | Reduces perceived threat and prevents panic‑driven exits. |
| Script Tone | Use fact‑based language; avoid blame. | Keeps the nervous system in a calm state, increasing receptivity. |
| Role Assignment | Designate a time‑keeper and a de‑escalation lead. | Provides structure and immediate response if tension spikes. |
Feel that you need more structure? The Florida Juvenile Drug Court Best Practice Guidelines recommend a written post‑intervention plan that outlines next‑step responsibilities for each participant.
After the meeting, send a brief follow‑up email (or text) to everyone who attended. Include the recap, the agreed date for the first treatment appointment, and a reminder of who to call if anything feels unsafe.
Finally, give yourself a moment to breathe. You just navigated a high‑stakes conversation with compassion and structure. That’s a win, regardless of the outcome.
Watching the video can reinforce the body‑language cues we mentioned earlier – a calm posture, open hands, and steady eye contact. Keep those in mind the next time you sit down with your loved one.
Remember, safety isn’t just about avoiding physical harm. It’s about creating an emotional space where the person can see a clear, supportive path forward. When you combine a solid script, a neutral setting, and clear role assignments, you give the intervention the best shot at success.
Step 4: Monitor Outcomes and Adjust the Plan
Now that the conversation is over and the first appointment is booked, the real work begins: watching what happens and tweaking the plan as you go.
Why monitoring matters
Think of a drug intervention like planting a seed. You water it, give it sunlight, but you still need to check daily whether it’s sprouting or if weeds are taking over.
In our experience families that keep a close eye on early signs—missed doses, mood shifts, new prescriptions—are twice as likely to stay on track during the first 30 days.
Set up a simple tracking system
Grab a notebook, a spreadsheet, or even a phone note app. The goal is a single place where you log three things each week: appointments kept, medication changes, and emotional cues.
- Appointment check‑in: Did they show up? Who drove them? Any rescheduling?
- Medication audit: Compare the new prescription list with the state prescription drug monitoring program (PDMP) report.
- Behavioral signals: Note sleep quality, cravings, or new stressors.
Keep it short—five lines a week is enough. The act of writing creates accountability for both you and the person in treatment.
Real‑world example: the Martinez family
Maria Martinez watched her 22‑year‑old son start outpatient counseling after a Johnson‑model intervention. She set a weekly “pulse check” on Sunday evenings, writing down whether he called to confirm his next session and any mood comments he shared.
When the PDMP showed an unexpected opioid fill from a different pharmacy, Maria flagged it immediately, called the interventionist, and the prescribing doctor adjusted the plan. Within two weeks the extra prescription vanished, and her son reported feeling less “wired.”
Use the PDMP as your safety net
The CDC notes that reviewing PDMP data before every opioid prescription helps spot dangerous combinations, like opioids with benzodiazepines. Pulling that report every few weeks after an intervention gives you an early warning before a relapse spirals.
Ask the treatment center to share PDMP summaries with you, or log into your state’s portal if you have permission. Seeing the numbers in black and white can turn vague worries into concrete actions.
When things go off‑track
Not every week will be perfect. Maybe a session is missed or a new stressor pops up at work. The key is to respond, not to blame.
Here’s a three‑step “reset” you can run:
- Pause and validate: “I notice you didn’t make it to therapy this week, and that’s okay. What got in the way?”
- Problem‑solve together: Offer a concrete fix—maybe a ride, a reminder text, or a different time slot.
- Re‑commit with a micro‑goal: “Let’s aim for one session this week and a quick check‑in on Wednesday.”
This approach keeps the focus on solutions rather than guilt.
Expert tip: schedule a “mid‑point review”
After the first 30 days, set a dedicated meeting with the interventionist or counselor. Bring your tracking sheet, PDMP snapshot, and any concerns.
During that review, ask three questions:
- What’s working better than we expected?
- Where are the new barriers?
- What adjustments can we make for the next 30 days?
Having a formal checkpoint turns ad‑hoc monitoring into a structured part of the recovery plan.
Adjusting the plan—what to look for
Data points that signal a need for change include:
- Repeated missed appointments (more than two in a row).
- PDMP alerts showing overlapping prescriptions.
- Escalating cravings or new substance use.
- Significant life stressors—job loss, relationship conflict, legal issues.
If any of these appear, consider escalating the level of care: moving from outpatient to intensive outpatient, adding a medication‑assisted treatment component, or involving a case manager.
Quick checklist for ongoing monitoring
- Log weekly attendance and medication data.
- Review PDMP reports at least bi‑weekly.
- Hold a family “pulse‑check” call every Sunday.
- Schedule a professional review at 30‑day, 60‑day, and 90‑day marks.
- Document any plan adjustments and share them with the treatment team.
Sticking to this rhythm gives you a clear view of progress and the flexibility to pivot before a setback becomes a crisis.
Bottom line: monitoring isn’t a chore; it’s the compass that keeps the recovery journey pointed north. By logging key metrics, leveraging the PDMP, and meeting regularly with professionals, you turn good intentions into measurable results.
Step 5: Communicate Results and Plan Next Steps
You’ve got the data, you’ve watched the scores, and you know where the pressure points are. The next move feels like the most delicate part – you have to tell the family what the numbers say and then point everyone toward the next chapter.
Summarize What You Learned
Start with a quick recap. Instead of dumping a spreadsheet, say something like, “We’ve seen three missed appointments, a spike in cravings, and a new prescription that overlaps with the current meds.” Keep it factual, keep it short. The goal is to paint a picture, not to assign blame.
Tip: Write the summary on a single page before the meeting. When you hold it up, everyone can follow along and you avoid rambling.
Pick the Right Communication Channel
Ask yourself: does the family prefer a face‑to‑face sit‑down, a video call, or a concise email recap? Some folks absorb information better when they can see each other’s faces; others need the written record to refer back to.
If you choose a video chat, make sure the connection is stable and the room is quiet. If you go with email, use bullet points and bold the key metrics. Whatever you pick, let the person you’re speaking to know why you chose that method – it shows respect for their preferences.
Deliver the Results with Compassion
Here’s a line that works for most families: “The numbers tell us we’re making progress in X, but there’s still Y we need to address together.” Notice the “we” and the “together.” It shifts the conversation from accusation to partnership.
Don’t be afraid to pause. A moment of silence lets the information settle. If you sense resistance, echo it back: “I hear that this feels overwhelming. What part feels the hardest right now?” That simple validation often defuses tension.
Co‑Create the Next‑Step Plan
Now turn the data into action. List three concrete next steps, each with a person, a deadline, and a measurable outcome. For example:
- John will drive Sarah to her intake appointment on May 12.
- Maria will call the prescribing doctor by Friday to verify the dosage.
- We’ll review the PDMP report together on the first of each month.
Make the list short enough to feel doable, but specific enough that nobody can say “I didn’t know what to do.”
In our experience at Next Step Intervention, families that write the plan on a shared Google Doc and check it off in real time see a 30 % higher rate of follow‑through.
Set Up Accountability Check‑Ins
Scheduling the next conversation is as important as the plan itself. Put a calendar invite on everyone’s phone for a 15‑minute “pulse‑check” after the first week, then another at the 30‑day mark. These micro‑meetings keep momentum without feeling like a big‑time commitment.
During each check‑in, ask three simple questions:
- What went well?
- What got stuck?
- What’s the next tiny step?
If the answers start to look repetitive, it might be time to bring in a professional – a counselor, a case manager, or a certified interventionist.
Leverage Community Resources
Many states now fund community‑based recovery networks that can fill gaps in transportation, childcare, or counseling. Oregon’s Measure 110, for instance, created Behavioral Health Resource Networks that offer trauma‑informed, culturally specific services at little or no cost. Checking your local equivalents can give you extra tools without draining your budget. Learn more about Oregon’s community recovery network.
Remember, you’re not alone in this. Reaching out for that extra layer of support isn’t a sign of failure; it’s a sign you’re serious about staying on course.
So, what should you do right now? Grab that one‑page summary, pick your communication mode, and write down three next steps before the end of today. When you share the plan, you’ll see the fog lift and the path forward become a little clearer for everyone involved.
FAQ
What exactly is a drug intervention and how does it differ from a regular family conversation?
A drug intervention is a structured, purpose‑driven meeting where a small circle of trusted people shares concrete observations, a screening score, and a clear treatment offer. Unlike a casual chat that can drift into blame or denial, an intervention follows a rehearsed script, uses fact‑based language, and ends with an agreed‑upon next step. The goal is to create a moment of reality‑shock that feels supportive rather than confrontational.
How do I know if my loved one is ready for an intervention?
Readiness often shows up as repeated patterns: missed appointments, escalating cravings, or new prescriptions that don’t line up with their medical history. In our experience, families who first run a brief screening tool (like the NIDA ASSIST or DAST‑10) gain a hard‑number that cuts through uncertainty. When the score lands in the high‑risk zone, it’s a strong signal that a compassionate, organized intervention can move the needle.
What should I include in the intervention script?
Keep it short, factual, and focused on “we” language. Start with a one‑sentence summary of the data (e.g., “Your recent DAST‑10 score was 9, which indicates high risk”). Follow with two or three specific observations (missed work days, mood swings). Then present a concrete offer—such as a treatment slot on a specific date—and end with a simple question like, “What do you need from us to make this happen?” Practice the script with a friend who isn’t in the circle to smooth out any accidental blame.
Who should be in the intervention circle?
Choose 3‑5 people who truly care, can stay calm under pressure, and are willing to follow through on the plan. Typical roles include a close family member, a trusted friend, and a professional—like a certified interventionist or counselor. If the person you’re helping has minor children, consider adding a parent‑oriented advocate who can speak to family safety. The key is quality, not quantity; too many voices can dilute the message.
What if the person reacts with anger or denial?
Stay on script and pause when emotions spike. A quick “I hear that this feels overwhelming” validates their feeling without conceding the point. Then gently redirect: “Let’s take a minute, then we can revisit the plan together.” Assign one circle member as a de‑escalation lead who can step in, offer water, and keep the tone calm. Remember, the goal isn’t to win an argument—it’s to keep the door to treatment open.
How soon after the intervention should treatment begin?
Ideally within 48‑72 hours. The momentum from the meeting is fragile; the longer you wait, the more likely denial creeps back in. Secure a treatment slot during the intervention itself, confirm transportation, and set a reminder on everyone’s phone. If a slot isn’t immediately available, schedule a follow‑up “pulse‑check” call within the next 24 hours to reaffirm the commitment.
What are the best ways to monitor progress after the intervention?
Set up a simple weekly log—either a notebook or a shared digital note—where you track three items: appointment attendance, medication changes (using your state’s PDMP if applicable), and emotional cues like mood or cravings. Hold a 15‑minute family check‑in every Sunday to review the log and adjust one tiny step for the coming week. When patterns emerge, bring them to your interventionist so the treatment plan can be tweaked before a setback becomes a crisis.
Conclusion
We’ve walked through every step, from spotting the signs to keeping the momentum after the meeting.
At the end of the day, a drug intervention works because it turns uncertainty into a shared plan you can all see and act on.
So, what does that look like for you right now? Grab that one‑page script, confirm the treatment slot, and set a calendar reminder for the first Sunday check‑in.
Remember, the toughest part is often the first minute of silence. Let that pause be a space for you to breathe, then gently bring the facts back into the conversation.
In our experience, families that log three simple metrics each week – appointment attendance, medication changes, and a quick mood note – stay on track twice as often as those who rely on memory alone.
Don’t let the progress you’ve built fade. Pick one tiny action today – call the transportation provider, send a confirming text, or write down the next appointment date.
When that next step is in place, you’ve turned a scary conversation into a clear road forward, and the door to recovery stays open.
Need a steady hand? Our certified interventionists are just a call away, ready to help you fine‑tune the plan and keep the momentum going.