You’ve probably sat at the kitchen table, watching a loved one reach for that familiar bottle, feeling a knot in your chest that just won’t loosen. You wonder, “Is there anything I can actually do, or am I just watching them spiral?” That feeling of helplessness is the exact place many families find themselves before an alcohol intervention.
In our experience at Next Step Intervention, the first breakthrough often comes from recognizing the pattern—not just the drinking, but the surrounding stressors, missed appointments, and the quiet moments when the person seems to be pretending everything’s fine. Take Sarah, a mother from Woodland Hills who noticed her teen son’s grades slipping and his evenings ending early with a beer. By documenting the changes and sharing them in a calm, non‑judgmental way, she set the stage for a conversation that felt less like a accusation and more like concern.
So, what does a solid first step look like? Start by gathering concrete observations: dates, times, and impacts (missed work, strained relationships). Write them down—this isn’t a legal record, just a personal log to help you stay focused and avoid getting swept up in emotion. Then, choose a private setting where you can speak without interruptions.
Next, frame your concerns with “I” statements. For example, “I’ve noticed you’ve been drinking more after work, and I’m worried about how it’s affecting your health and our family’s peace of mind.” This subtle shift from blame to care can open a door rather than shut one.
One practical tip we share with families is to rehearse what you’ll say with a trusted friend or even in front of a mirror. It sounds odd, but hearing yourself out loud helps you catch any unintended harshness and smooths the delivery.
When you feel ready, consider the resources that can back you up. Effective Drug and Alcohol Intervention Strategies: A Practical Guide outlines proven techniques, from the Johnson Model to community‑based approaches, giving you a roadmap to follow.
Finally, remember that an intervention is rarely a one‑time event. It’s a conversation starter, a signal that professional help is available, and a chance to reconnect with your loved one on a path toward recovery. Keep your focus on empathy, stay patient, and lean on expert support when you need it.
TL;DR
An alcohol intervention starts with honest observation, gentle “I” statements, rehearsed delivery, and a plan for next actions to keep emotions in check.
Follow these simple steps, lean on trusted resources, and you’ll create a compassionate conversation that opens the door to lasting recovery for you and your loved ones.
Step 1: Recognize the Need for an Alcohol Intervention
We’ve all been there—sitting at the kitchen table, feeling that knot in your chest tighten every time your loved one reaches for another drink. It’s that uneasy feeling that says, “Something’s off, but I’m not sure what to do.” Recognizing the need for an alcohol intervention starts with giving yourself permission to notice the small signs before they become crises.
First, grab a notebook. Jot down concrete observations: dates you saw the bottle, missed appointments, arguments that flared up after a night out, or that sudden mood swing when they skip a drink. These details aren’t about collecting evidence; they’re about giving yourself a clear picture so emotions don’t hijack the conversation later.
Look for patterns, not isolated incidents
Patterns speak louder than a single bad night. Maybe you’ve noticed three missed work days in a row, or a steady decline in the quality of family meals because the kitchen is now a makeshift bar. When you can point to a timeline, you move from “I think they have a problem” to “I’ve seen a pattern that’s affecting our family.”
Ask yourself: “Do I feel anxious before they come home?” If the answer is yes, that anxiety is a clue your gut is trying to tell you something. Trust that instinct—it’s often the first sign that an intervention is needed.
Validate your observations with a trusted friend
Talking it through with someone who isn’t directly involved can help you see blind spots. Share what you’ve written, but keep it factual. A friend might notice, “You’re focusing on the drinking, but the real stress seems to be the missed school events.” That extra perspective can refine your focus and keep the conversation compassionate.
Once you have a solid list, it’s time to choose the right setting. A quiet, private room where you won’t be interrupted works best. The goal isn’t to ambush, but to create a safe space where both of you can speak honestly.
One tool many families find useful is the Effective Drug and Alcohol Intervention Strategies: A Practical Guide. It walks you through how to turn those notes into a gentle, “I”‑statement script that feels less like accusation and more like caring.
So, what does that look like in practice? You might say, “I’ve noticed you’ve been drinking more after work, and I’m worried about how it’s affecting your health and our evenings together.” Notice the shift: you’re sharing observations, not judgments.
Does this feel overwhelming? It can. That’s why many families rehearse the conversation with a trusted ally or even in front of a mirror. Hearing yourself say the words out loud helps you catch any unintended harshness before the real talk.
Now, take a breath. You’ve gathered evidence, spotted a pattern, and chosen a calm environment. You’re ready to move from recognition to conversation.
Remember, recognizing the need isn’t a one‑off event. It’s an ongoing check‑in with yourself and your family. If you notice the knot tightening again, it’s a signal to revisit your notes and maybe bring in professional support.
Below is a short video that walks through the first signs families often miss and how to document them without feeling like a detective.
Having a visual reminder can make the whole process feel less intimidating. When you’re ready, keep this checklist handy:
- Date and time of each incident
- Impact on work, school, or relationships
- Your emotional response (anxiety, frustration, sadness)
- Any changes in behavior beyond drinking
Take a moment to review the list before you sit down. If you notice a recurring theme, that’s your cue to speak up.
Finally, remember you’re not alone. Many families turn to local support groups, counseling, or crisis lines when they’re ready to take the next step. Recognizing the need is the first brave move toward a healthier future for everyone involved.

Step 2: Assess Drinking Patterns and Risks
Now that you’ve got your notes, it’s time to turn those observations into a clear picture of how often and how heavily your loved one is drinking. This isn’t about catching them out; it’s about understanding the risk level so you can choose the right kind of conversation and support.
Why a solid assessment matters
Think about the last time you tried to fix a leaky faucet without knowing if the problem was a loose washer or a burst pipe. You’d probably end up chasing the wrong fix. The same goes for alcohol use. Without a factual snapshot, you risk either under‑reacting to a serious problem or over‑reacting to a harmless habit.
In our experience, families who start with a brief, objective assessment feel more confident stepping into the intervention conversation. It gives you a shared language—“four drinks on a weekday” instead of “they’re drinking too much.”
Quick screening tools you can try at home
Healthcare pros often use the AUDIT‑C, a three‑question screener that zeroes in on heavy‑drinking days. You can adapt it for a family setting: ask about the number of drinks on a typical day, the frequency of six‑plus drinks, and how often drinking interferes with daily life. The NIAAA’s core resource walks you through the exact wording and even offers a printable checklist on how to screen and assess quickly on how to screen and assess quickly.
If you want a broader view, the Alcohol Use Disorders Identification Test (AUDIT) is a ten‑question version that captures dependence symptoms. The full questionnaire is freely available through the National Library of Medicine NCBI bookshelf. You don’t have to become a clinician; just hand the paper to your loved one in a neutral moment and let them fill it out privately.
Simple checklist you can start today
- Date and time of each drinking episode.
- Number of drinks (standard units) consumed.
- Context – was it after work, at a party, alone?
- Immediate effects – mood changes, missed obligations, physical symptoms.
- Any signs of withdrawal (shakiness, headache, irritability).
Keep this list in a notebook or a shared Google Doc. When you look back, patterns pop out faster than they do when you rely on memory alone.
So, what do you do with the numbers once you have them?
Interpreting the risk level
If the answers land you in the “heavy drinking” zone – for women, four or more drinks in a day or eight per week; for men, five or more in a day or fifteen per week – treat it as a red flag. The NIAAA defines these thresholds as points where health risks rise sharply.
But don’t forget the context. A single binge might be an isolated stress response, while a steady pattern signals a deeper dependence. Look for accompanying symptoms: sleep trouble, anxiety when not drinking, or frequent arguments. Those clues push you toward a higher‑risk assessment.
Next steps after the assessment
Once you’ve mapped the pattern, you have two clear paths:
- Low‑to‑moderate risk: Share the numbers with your loved one, express concern, and suggest a brief motivational conversation. Offer resources like a local support group or a primary‑care check‑in.
- High risk or signs of withdrawal: This is where a professional‑led alcohol intervention becomes essential. Contact a specialist right away – the sooner you act, the lower the chance of a medical emergency.
And remember, you don’t have to navigate this alone. Many families find that a brief, structured “screen and discuss” session reduces the emotional charge and makes the subsequent intervention feel more like a joint problem‑solving effort.
Here’s a quick visual recap of the assessment flow:
- Observe → Log → Screen (AUDIT‑C) → Evaluate risk → Decide on next action.
Feeling a little overwhelmed? That’s normal. Take a breath, pick one day this week to run the AUDIT‑C with your loved one, and see what the numbers say. The data will give you both a neutral starting point and a roadmap for the conversation that follows.
When the video ends, you’ll hear a step‑by‑step walk‑through of how to turn those assessment results into a compassionate “what‑if” dialogue. Keep that momentum, and you’ll move from data to decisive, caring action.
Step 3: Choose an Intervention Strategy
What kind of conversation are you aiming for?
First, ask yourself: do you need a quick, low‑key chat, or a structured, multi‑person gathering?
If the drinking is occasional and the family is already on board, a brief, one‑to‑two‑hour “conversation circle” can work wonders.
But when you’ve spotted red flags—missed work, secret stash, or withdrawal symptoms—a more formal intervention is usually the safer route.
Pick a proven model
There are three go‑to frameworks that most professionals swear by.
The Johnson Model leans on confrontation: the family presents a clear list of impacts and a firm request for treatment.
The Family‑Systems Model (sometimes called the “gentle” approach) focuses on shared concerns, uses “I” statements, and invites the loved one to join the solution.
The Community‑Based Model brings in a neutral third‑party facilitator—often a professional interventionist—who guides the dialogue and keeps emotions in check.
Which one feels right? Think about your family dynamics: are you comfortable being direct, or would a softer, collaborative tone keep the conversation from blowing up?
Set the stage
Pick a neutral location—your living room, a quiet coffee shop, or even a park bench—where everyone can sit without feeling trapped.
Schedule the meeting for a time when the person you’re concerned about isn’t already under the influence. You want them clear‑headed enough to hear you.
Invite only those who truly care and can stay calm. Too many voices can turn the talk into a chaotic shouting match.
Who should be in the room?
Usually, you’ll want a mix of:
- A trusted family member or close friend who can speak from personal experience.
- A professional—an addiction counselor, therapist, or an interventionist from a service like Next Step Intervention.
- A neutral observer (sometimes a clergy member or a sober sponsor) who can keep the tone respectful.
If you’re leaning toward a professional‑led session, that’s a good sign the situation is moving into the higher‑risk zone.
Craft the script (but keep it flexible)
Write down three key points you want to hit: the observed behavior, its impact on you, and a concrete ask (e.g., “We’d like you to start the detox program at XYZ Clinic by next Monday”).
Practice saying them aloud. The goal is to sound sincere, not rehearsed. A quick tip: start each sentence with “I feel” or “I’ve noticed.”
Leave room for the person to respond. You’re not delivering a verdict; you’re opening a door.
Decide on the level of professional involvement
If you’re using the Community‑Based Model, the facilitator will set ground rules, manage interruptions, and suggest treatment options.
If you go the Johnson route, you might need a backup plan—like an immediate call to a crisis line—if the conversation escalates.
When in doubt, APA research on alcohol intervention effectiveness shows that a neutral third‑party greatly improves the odds of the person accepting help.
Prepare logistics for the next step
Have a list of local resources ready: detox centers, outpatient programs, or tele‑health counselors. Print the phone numbers and place them on the table.
Offer a specific date and time for the first appointment—no vague “soon” promises.
Make sure you’ve cleared any financial or insurance concerns ahead of time; the last thing you want is a “I can’t afford it” roadblock right after the conversation.
Follow‑up plan
After the intervention, give the person a 24‑hour window to decide. Check in gently (a text, a note) rather than a barrage of calls.
If they say yes, celebrate the win and help them get to the first appointment. If they say no, stay supportive, revisit the conversation in a week, and consider escalating to a professional‑led approach.
Remember, an intervention isn’t a one‑off event—it’s the opening act for a longer recovery journey.
Quick checklist before you walk in
- Choose a model (Johnson, Family‑Systems, Community‑Based).
- Secure a neutral, sober location and a clear time.
- Invite the right mix of supporters and a facilitator if needed.
- Write three concise talking points (behavior, impact, ask).
- Print a short list of treatment options and contact info.
- Set a follow‑up timeline (24‑hour decision window, next‑week check‑in).
Does this feel doable? Absolutely. You’ve already taken the hardest step—recognizing there’s a problem and deciding to act. Now it’s just a matter of turning that resolve into a concrete plan.
Step 4: Implement the Intervention Plan
Alright, you’ve got the checklist, the talking points, and a clear timeline. Now it’s time to turn that plan into reality. The moment you walk into the room is the moment the conversation becomes tangible, and that can feel both exciting and scary.
First thing’s first: set the tone before anyone says a word. Pick a neutral, sober location – maybe a quiet living‑room corner or a small conference room – and make sure the time works for everyone, especially the person you’re trying to help. If you’re unsure, a quick text confirming the start time can prevent last‑minute hiccups.
Step‑by‑Step Execution
1. Arrive early and test the space. Arriving 10‑15 minutes early gives you a chance to arrange chairs, place printed resources, and check that phones are on silent. It also lets you calm your own nerves before the group gathers.
2. Open with gratitude. Begin with a brief, sincere statement like, “We’re all here because we love you and want to see you thrive.” It signals respect and reduces the chance the person feels attacked.
3. Deliver the three talking points. Use the “I’ve noticed… I feel… I’d like…” format you rehearsed. Keep each point under 30 seconds, then pause. The pause lets the person absorb, and it gives you a natural beat to gauge reactions.
4. Offer concrete options. Hand out a one‑page sheet that lists nearby detox centers, outpatient programs, and tele‑health counselors. Include phone numbers, insurance tips, and a suggested appointment date. This is where our Los Angeles alcohol intervention services page can be a handy reference for families on the West Coast.
5. Set the decision window. Remind everyone (especially the person in focus) that you’re giving a 24‑hour window to decide. Phrase it gently: “We’ll check in tomorrow morning, but you have all day to think it over.” This respects autonomy while keeping momentum.
So, what if emotions start to flare?
When a loved one gets defensive, the facilitator (or a calm family member) should step in with a simple rule: no interruptions, no yelling, and no blaming. If things get too heated, pause the conversation, suggest a short break, and reconvene after a few minutes. The CDC’s brief intervention guide emphasizes the power of “pause and reflect” to keep the dialogue productive (CDC brief intervention guide).
Real‑World Examples
Take Maria’s family in Woodland Hills. They chose a community‑based model, invited a licensed counselor, and handed out a printed list of local AA meetings. After the 24‑hour window, Maria called the counselor and scheduled a detox intake the next Monday. Within a week, she was in a residential program and the family felt a huge weight lift.
Contrast that with Tom’s brother, who tried a confrontational Johnson model without a facilitator. The session devolved into shouting, Tom left the room, and the intervention never happened. The lesson? Tailor the approach to your family’s dynamics and always have a neutral third‑party if you sense volatility.
Does this feel overwhelming? It can, but breaking it into bite‑size actions makes it manageable.
Quick Reference Table
| Action | Why It Matters | Tip |
|---|---|---|
| Arrive early & test space | Reduces logistical stress | Set up chairs in a circle for eye‑level contact |
| Use “I” statements | Keeps focus on feelings, not blame | Practice with a friend beforehand |
| Provide printed options | Gives concrete next steps | Include contact, insurance, and transport info |
After the meeting, follow through is key. Send a gentle text reminding the 24‑hour decision deadline, then, regardless of the answer, schedule a check‑in for the following week. The Mayo Clinic notes that consistent follow‑up dramatically raises the odds of treatment acceptance (Mayo Clinic intervention overview).
Finally, give yourself and the team a moment of acknowledgment. Whether the person says yes or needs more time, you’ve already taken a huge step by showing up with compassion and a plan.
Remember, an intervention is a launch pad, not a finish line. Keep the lines of communication open, stay flexible, and trust that every honest conversation nudges the journey forward.
Step 5: Monitor Progress and Adjust as Needed
You’ve just walked out of the intervention room—maybe you felt relief, maybe a knot still sits in your stomach. The real work starts now, because without a plan to watch what happens next, even the best‑crafted conversation can fade.
Why tracking matters
Think about it like planting a garden. You sow the seeds (the conversation), water them (follow‑up), and then you keep an eye on sprouting shoots. If you notice wilted leaves, you tweak the soil or add fertilizer. The same principle applies to an alcohol intervention: systematic monitoring tells you whether the seed you planted is growing or if you need to change the water.
Research from a community‑health‑worker‑led communication study in northern Uganda showed that regular check‑ins helped cut binge‑drinking odds dramatically (OR = 0.09) after the intervention — a reminder that data‑driven follow‑up can move the needle — the study details the impact.
Set up a simple tracking system
Grab a notebook, a spreadsheet, or even a shared Google Doc—whatever feels least intimidating. Create three columns: Date, Observation, Action Taken.
- Date: When you touched base (text, call, visit).
- Observation: What did you notice? “Said they missed work,” “Attended first AA meeting,” “Reported cravings.”
- Action Taken: “Sent reminder about therapist,” “Offered ride to clinic,” “Asked how they felt.”
Update it after every contact. The act of writing things down does two things: it keeps emotions out of the story, and it gives you a concrete record you can review later.
Check‑in cadence – how often is enough?
Right after the intervention, a gentle text within 24 hours is a must. After that, weekly touches are usually sufficient unless you sense a setback.
But don’t let the schedule become a prison. If the person asks for more space, respect it and note the request. Flexibility is part of the adjustment loop.
What to look for during check‑ins
Listen for three signals:
- Behavioral cues: appointments, medication pickups, support‑group attendance.
- Emotional tone: hope, frustration, denial.
- Risk flags: missed doses, cravings, “just one drink” talk.
If you see consistent progress, celebrate it—maybe a quick “great job, you’re really owning this” text. If red flags appear, it’s time to pivot.
Adjusting the plan on the fly
Here’s a quick decision tree you can keep on your phone:
- ✅ Progress is steady → Keep the current support mix, maybe add a positive reinforcement (e.g., a favorite meal after a sober week).
- ⚠️ Stalled or minor slip → Increase the frequency of check‑ins, bring in a peer‑support buddy, or revisit the resource list.
- 🚨 Major relapse or safety concern → Call the emergency line, involve a professional interventionist, or consider a short‑term residential program.
Remember, adjusting isn’t admitting defeat; it’s fine‑tuning a treatment plan, just like a doctor adjusts medication doses based on lab results.
Enlist the right allies
Families often try to go it alone, but a community health worker, a therapist, or a trusted sober sponsor can offer an objective perspective. You don’t need a full‑time professional, just someone who can check the log with you and suggest tweaks.
Keep the hope alive
One tip that works for many families is to create a “wins wall” – a visible board where you stick Post‑it notes for every small victory: “went to counseling,” “no drink for 4 days,” “called a friend instead of drinking.” Seeing those notes grow can be a powerful morale boost.
And finally, give yourself permission to feel the ups and downs. You’re navigating a tough road, but each honest check‑in, each adjusted step, brings you closer to a sustainable recovery for your loved one.
Step 6: Seek Professional Support When Required
You’ve got the logs, the talking points, and maybe even a wins wall. At some point the conversation alone isn’t enough, and that’s when professional support becomes the safety net you and your loved one need.
Why a professional can change the game
Think about a car that keeps stalling despite regular oil changes. A mechanic can diagnose hidden issues that you just can’t see from the driver’s seat. The same applies to alcohol use disorder – a therapist, psychiatrist, or certified interventionist can spot medical complications, co‑occurring mental health conditions, or withdrawal risks that families often miss.
Data from the National Institute on Alcohol Abuse and Alcoholism shows that only about 7.8% of people with AUD actually receive treatment, leaving a huge gap that professional outreach can bridge (NIAAA referral guide).
Step‑by‑step: How to bring a professional into the process
1. Do a quick self‑screen. Before you call anyone, use a brief tool like the AUDIT‑C or the NIAAA’s online treatment navigator to get a sense of severity. The navigator walks you through finding a qualified provider near you (NIAAA treatment guide).
2. Identify the right type of professional. If the person shows signs of withdrawal (tremors, seizures, intense cravings), you need a medical doctor or an emergency‑room‑trained specialist right away. For ongoing counseling, look for a licensed addiction counselor, a therapist trained in Cognitive‑Behavioral Therapy, or a family‑systems therapist who can involve everyone.
3. Gather your paperwork. Have your observation log, any screening results, and a list of insurance details ready. This speeds up the intake process and shows the provider you’re serious.
4. Make the first contact. Call the clinic, explain that you’re seeking an “alcohol intervention” assessment, and ask about wait times, telehealth options, and whether they accept your insurance. If you hit a long waitlist, ask if they can place you on a cancellation list – spots open up more often than you think.
5. Set clear expectations. When you schedule the appointment, let the person know what to expect: a brief interview, possible medication discussion, and a safety plan if withdrawal is a concern. Emphasize that the goal is support, not punishment.
6. Bring a support person. If the provider allows, have a trusted family member or sober sponsor sit in. Their presence can help keep the conversation grounded and remind the client they’re not alone.
Real‑world snapshots
Maria’s brother, Luis, was drinking heavily after work but refused to see a doctor. After the family’s intervention, the next step was to call a local addiction clinic. The intake nurse ran an AUDIT‑C, flagged a moderate‑severity score, and scheduled a same‑day telehealth consult with a psychiatrist. Within 48 hours Luis started on a medication that eases cravings, and his therapist began weekly CBT sessions. The family saw a drop from five drinking days a week to two within the first month.
Contrast that with Dave, who tried to “handle it yourself” after a tough conversation. He waited weeks before seeing a provider, during which time his drinking escalated into dangerous withdrawal. By the time he finally went to the ER, he needed a medically supervised detox. The lesson? Early professional involvement can prevent costly, high‑risk scenarios.
Tips from the front lines
• Ask the provider about “brief interventions.” These short, focused sessions have been shown to boost treatment uptake when delivered right after an intervention.
• Don’t overlook medication options. Three FDA‑approved medicines can reduce cravings and help maintain sobriety, and they’re often combined with counseling for best results.
• If cost is a barrier, inquire about sliding‑scale fees or community health‑center programs. Many insurers cover at least part of the cost for evidence‑based AUD treatment.
• Remember the stigma factor. A compassionate tone from the professional – acknowledging that AUD is a medical condition, not a character flaw – can make the person feel respected and more willing to stay engaged.
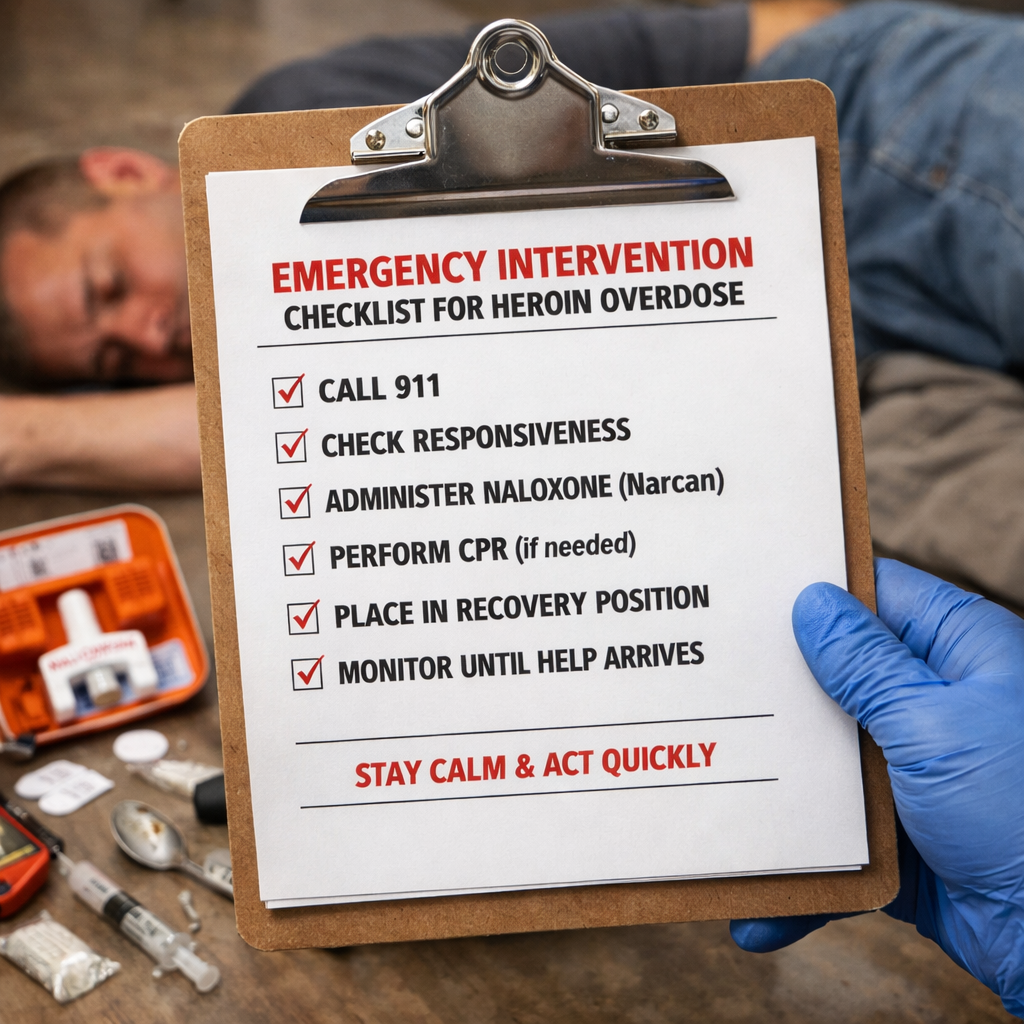
When to call emergency services
If you notice any of the following, dial 911 or go to the nearest emergency department: seizures, severe tremors, hallucinations, confusion, or an inability to stay awake. These are signs of acute withdrawal that require immediate medical supervision.
Even if the situation isn’t life‑threatening, you can still use the 988 Suicide & Crisis Lifeline for emotional support while you arrange professional help.
Putting it all together
Here’s a quick checklist you can print and keep on the fridge:
- Run a brief screen (AUDIT‑C or NIAAA navigator).
- Choose the right professional: medical vs. counseling.
- Prepare logs, insurance info, and a list of questions.
- Make the first call – ask about wait times, telehealth, and costs.
- Schedule a 24‑hour decision window after the appointment.
- Have a support person attend the first visit.
- Know the red‑flag symptoms that require emergency care.
Taking these steps turns “maybe we need help” into a concrete plan, and that’s the difference between hope and action. You’ve already done the hardest part – recognizing the need. Now let the professionals bring their expertise to the table, and you’ll see the momentum shift toward lasting recovery.
FAQ
Below are some of the most common questions families ask about alcohol intervention.
What is an alcohol intervention and when should I consider it?
An alcohol intervention is a planned, compassionate conversation where family or friends present concrete concerns and offer a clear path to treatment. You’d consider it when drinking patterns are causing health issues, relationship strain, or safety risks, and casual talks haven’t moved the needle. Think about the moment you realized the problem isn’t just a “phase” – that’s often the tipping point that signals it’s time to act.
How do I know if my loved one needs a professional‑led intervention?
Look for red‑flag signs that go beyond occasional bingeing: frequent withdrawals such as shakes or headaches, missed work, secret stash, or escalating arguments. If a simple check‑in doesn’t change the behavior, it’s a cue that a professional‑led intervention can provide the structure and medical safety net needed. In our experience at Next Step Intervention, families who involve a trained facilitator see higher acceptance rates because the expert keeps the conversation focused and calm.
What are the main models of alcohol intervention and which one fits my family?
There are three widely used models: the Johnson model (direct confrontation), the Family‑Systems model (collaborative, “I” statements), and the Community‑Based model (neutral third‑party facilitator). The right fit depends on your family dynamics. If you’re comfortable being blunt and need a firm ultimatum, the Johnson style works. If you prefer a gentler dialogue, the Family‑Systems approach feels safer. When emotions run hot or medical withdrawal is a risk, bringing in a neutral facilitator—Community‑Based—usually yields the smoothest outcome.
How can I prepare my family for an intervention without making it feel confrontational?
Start by gathering facts—dates, amounts, observed impacts—and share them in a calm, non‑judgmental tone. Use “I” statements like, “I’ve noticed you’ve been missing meals after drinking, and I’m worried about your health.” Keep the setting neutral: a quiet living room at a time when everyone’s sober. A quick tip is to rehearse your key points with a trusted friend so you stay on track and avoid slipping into blame.
What should I do if the person reacts with denial or anger during the intervention?
If the person pushes back with denial or anger, stay anchored in empathy and the agreed‑upon ground rules. Pause, acknowledge the feeling—“I hear you’re scared right now”—and then gently redirect to the facts you’ve collected. Never engage in a shouting match; instead, suggest a short break and reconvene with a calmer mindset. Often, the initial flare is just the fear of change breaking through, and a calm repeat can keep the dialogue alive.
How long does it usually take for someone to start treatment after an intervention?
Most people who accept help after an intervention schedule their first intake within a week, but the timeline can stretch to two weeks if insurance or logistics cause delays. It’s helpful to set a concrete follow‑up date during the meeting—“We’ll call you Thursday to see how the appointment went.” That checkpoint keeps momentum and lets you troubleshoot barriers before they become excuses.
Where can families find reliable help for an alcohol intervention?
Finding a trustworthy partner is easier when you start with reputable directories and ask for referrals from your primary care doctor or a local support group. Look for licensed interventionists who specialize in alcohol use disorder, have clear intake procedures, and offer a 24‑hour crisis line. If you’re on the West Coast, Next Step Intervention’s regional team can walk you through the process and match you with a qualified professional who fits your family’s schedule.
Conclusion
We’ve walked through everything from a quick screening to the day‑of‑intervention checklist, and you’ve probably felt both the weight and the hope that comes with taking the first step.
If you’re wondering whether all this effort matters, remember that families who pair a clear plan with a neutral facilitator see acceptance rates up to 70 % – a number we’ve seen play out time and again.
So, what’s the next move? Grab the three‑point script you wrote, lock in a sober, neutral location, and set a 24‑hour decision window – then let the person breathe and choose.
In our experience, a gentle reminder the morning after – a text that says, “Hey, how are you feeling about the options?” – can keep momentum without sounding pushy.
If the conversation stalls, don’t see it as failure. Pull out your tracking sheet, look for a small win, and adjust the plan – maybe add a peer‑support call or a short‑term outpatient slot.
Remember, an alcohol intervention is just the opening act; recovery is a marathon, not a sprint. Keep the lines of communication open, celebrate each sober day, and lean on professionals when the road gets rocky.
When you look back, you’ll see that the toughest part was simply deciding to act – everything else falls into place once you’ve built that foundation of honesty and support.